Bile leak after laparoscopic cholecystectomy occurs in 1-4% of cases [1,2,3] and is generally due to a minor biliary duct injury, although it can sometimes be due to a major duct injury.
The cystic duct stump and small peripheral right hepatic ducts within the liver bed account for most bile leaks. These settle either spontaneously or with the help of Endoscopic Retrograde Cholangio Pancreatography with or without Endoscopic Retrograde Cholangio Pancreatography (ERCP)
ERCP is similar to gastroscopy, but uses a modified scope with side viewing tip, and allows visualisaton of the common bile duct opening in the second part of the duodenum. This can be injected with dye to provide x-ray images of the Common Bile Duct, to determine if there is a leak or retained stone.
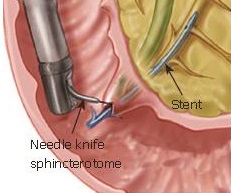
ERCP also allows the passage of a basket or balloon to remove a retained common bile duct stone. It also allows sphincterotomy – the cutting of the sphincter of Oddi (a muscular valve-like opening of the Common Bile Duct into the duodenum) to be performed. This involves use of a needle knife sphincterotome. The end result is a reduction in CBD bile pressure. In addition a plastic stent can be placed via the sphincter of Oddi, with half of the stent in the Common Bile Duct and half in the duodenum. This keeps the sphincter of Oddi open and freely draining.
1. Brooks DC, Becker JM, Connors PJ, Carr-Locke DL. Management of bile leaks following laparoscopic cholecystectomy. Surg Endosc. 1993;7:292–5.
2. Kozarek RA, Traverso LW. Endoscopic stent placement for cystic duct leak following laparoscopic cholecystectomy. Gastrointest Endosc. 1991;37:71–3.
2. Ponsky JL. Complications of laparoscopic cholecystectomy. Am J Surg. 1991;161:393–5